Treatment for acute coronary syndrome varies. It ranges from medications to surgery methods to restore blood flow through your heart.
Medications can help to relieve chest pain and improve blood flow. Some medications your doctor could prescribe to you are aspirins, beta-blockers, cholesterol-lowering drugs etc. Procedures like angioplasty and stenting could also be recommended. Depending on the severity, the doctor could also recommend coronary artery bypass surgery.
1. Coronary Angioplasty and Stenting
Coronary artery narrowings may be treated using either medications that reduce the heart's demand for blood, or by procedures aimed at increasing the heart's blood supply. One of the two most common methods to increase the blood supply is Coronary Angioplasty, sometimes abbreviated as PTCA (Percutaneous Transluminal Coronary Angioplasty).
PTCA offers a non-surgical alternative to Coronary Artery Bypass Surgery.
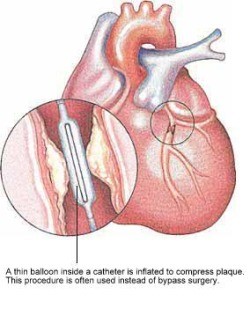
In PTCA, a balloon mounted on a thin tube (a catheter) is advanced into your coronary artery until it lies within the narrow area. The balloon is then inflated at high pressure, often a few times, to dilate the narrowing. Upon balloon deflation, the arterial narrowing is often significantly reduced.

A stent is a small metal coil to provide support to the narrowed segment of the coronary artery after angioplasty, preventing the artery from collapsing and reducing the likelihood of the narrowing recurring. Modern stents are made of stainless steel or a cobalt chromium alloy and are inert to the body. Some stents also have a medication coating and these may be preferred in certain situations to further reduce the chance of repeat narrowing of the heart arteries. Nowadays, stents are frequently placed directly over the narrowed segments (direct stenting) without prior balloon dilatation.
1.1. What to expect?
Before going through a PTCA, a coronary angiogram is done first to provide a 'roadmap'. Undergoing PTCA is also very similar to having a coronary angiogram procedure.
- First, you will be injected with local anaesthetic.
- A plastic tube known as sheath is inserted in a large artery in the groin or wrist. Through this sheath, a catheter is advanced to the mouth of the narrowed coronary artery.
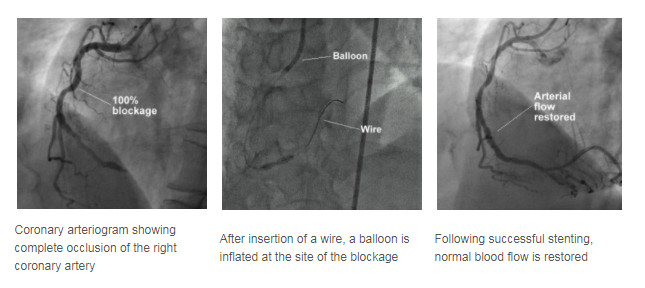
- A thin wire is then threaded through the catheter and positioned in the coronary artery.
- Over this wire, the balloon catheter is pushed into the artery and the balloon positioned over the area of narrowing.
During balloon inflation, you may experience some chest discomfort, and you should report this to your attending cardiologist. Stenting is carried out in a similar manner. The procedure may take from 1 to 2 hours or more depending on the complexity of the diseased artery.
Following the successful PTCA, you will be monitored in a special monitoring ward. During this period, the sheath may be kept in your groin artery for 4 to 5 hours. However, the sheath may be removed immediately after the procedure if the situation allows. After the sheath is removed, the puncture site will be compressed for about 30 minutes to ensure that there is no bleeding.
You will have to remain in bed for several hours or until the following day to ensure the puncture site is sufficiently healed before walking. Your cardiologist will determine how long you need to stay in bed before you can walk around. Following that, some blood tests and ECGs will be performed to monitor your condition. If there are no complications, most patients can be discharged on the same day or the day after.
1.2. What to prepare?
- Please inform your doctor of any allergy, in particular, allergies to seafood, iodine, X-ray contrast medium and pain relieving medications.
- Please inform your doctor if you have a history of peptic ulcer disease, recent strokes, or blooding tendencies.
- If you are suffering from diabetes mellitus and you are taking a medication called metformin, please inform your doctor and you would need to stop this particular medication for at least 2 days before and after Angiography.
- After being discharged, you will be given two anti-blood clotting medications – aspirin and either ticlopidine or clopidogrel. For the latter two medicines (ticlopidine or clopidogrel), your cardiologist will advise you on the optimal length of time you should continue taking them. This can range from one month to one year. However, aspirin should be taken indefinitely to prevent future heart attacks, unless instructed otherwise by your cardiologist.
1.3. What are the success rates?
The success rate of Coronary Angioplasty is usually about 95%, depending on the nature of your coronary narrowing. However, in about 5% of cases, the procedure may be unsuccessful and the artery remains narrowed. In very few patients (about 1%), urgent bypass surgery may be required if the procedure is complicated.
There is a possibility of a recurrence of the narrowing of the coronary artery in the 6 months following the initial successful angioplasty or stenting, and you would usually feel a chest discomfort should it happen. If you feel a chest pain, you should seek medical attention immediately and inform your doctor.
1.4. What are the potential risks or complications?
Major complications like heart attacks, abnormal heart rhythm, stroke and death occur in less than 1% of the patients undergoing PTCA.
Less serious complications like bleeding from the puncture site, bruising and swelling of the puncture site, and blood clot formation in the artery where the sheath is inserted occur in 1-3% of the patients.
Overall, the procedure is very safe and well-tolerated.
1.5. Home Care
As a patient:
- Resume normal daily activities.
- Notify the doctor at once if you experience bleeding or increased bruising at the puncture site; or when you experience a recurrence of symptoms, such as breathlessness or decreased exercise tolerance.
- Comply with regular follow-up visits.
