
Palliative care focuses on improving quality of life for individuals with serious or life-limiting illnesses. It helps relieve discomfort, provides emotional and practical support, and empowers patients and their families to make informed care decisions.
Compassionate Discharge: Spending Final Moments at Home
At NUHCS, we believe that patients should have the option to spend their final moments at home, surrounded by loved ones. Our compassionate discharge process helps make this possible.
Our Palliative Care Resource Nurse (PCRN) works closely with doctors, nurses, and families to:
This process reflects NUHCS’ commitment to providing dignified, patient-centered care, allowing patients to be in a familiar environment with their loved ones, during their final days.
Partnership with Home Hospice Services
NUHCS works closely with Methodist Welfare Services (MWS) Home Hospice to ensure seamless care for heart failure patients who need palliative support at home.
Dr Perryn Ng, Consultant, Department of Cardiology, NUHCS, leads our cardio-palliative initiatives and has worked closely with MWS to strengthen our partnership. MWS serves the western region of Singapore, which includes NUHCS patients. This collaboration allows for continuity of care.
How This Helps Patients
By combining NUHCS’ heart care expertise with MWS’ home hospice experience, we help heart failure patients receive personalized, compassionate care in their final stages of life.
Supporting Patients and Families Through the Palliative Journey
At NUHCS, we are here to support you and your loved ones every step of the way during this challenging journey. Our Palliative Care Resource Nurse program ensures that your loved one receives compassionate, individualized care, addressing their physical, emotional, and spiritual needs. We are committed to making this difficult time as comfortable and dignified as possible, providing guidance and support for you and your family throughout. If you or a loved one are considering palliative care, please consult with your healthcare team for guidance and support.
Palliative care plays a vital role in the holistic management of patients with advanced cardiac conditions. It focuses on improving quality of life by addressing symptoms, facilitating goals-of-care discussions, and ensuring compassionate end-of-life care. For healthcare providers, integrating palliative principles into cardiology is essential to delivering patient-centered care that aligns medical interventions with individual values and preferences.
Cardio-Palliative Multidisciplinary Teaching (MDT)
The integration of palliative care into cardiology is crucial in the management of patients with advanced heart failure and other serious cardiac conditions. Recognizing this need, the Cardio-Palliative Care Initiative was formally introduced in August 2021, marking a significant milestone in embedding palliative principles within cardiology practice.
A key step in this journey was the first Cardio-Palliative MDT, which served as a platform to foster awareness and education among healthcare providers. This session brought together experts from palliative medicine, cardiology, and nursing, emphasizing the importance of a collaborative approach. Leading the discussion were Adj A/Prof Noreen Chan, Senior Consultant and Dr Sara Ho, Consultant, both from the Division of Palliative Care, National University Cancer Institute (NCIS), Dr Perryn Ng, Consultant, Division of Cardiology, Department of Medicine, NUHCS @ NTFGH, and Juvena Gan, Advanced Practice Nurse (APN), NUHCS.
The MDT sessions are case-based discussions, illustrating real-world applications of palliative care principles in cardiology. Through these cases, participants explored topics such as symptoms management, goals-of-care discussions, Advance Care Planning, and end-of-life discussions for patients with advanced cardiac diseases. The sessions also addressed the role of palliative screening in identifying patients who may benefit from early supportive care interventions.
By facilitating dialogue between cardiologists, palliative care specialists, nurses and allied health professionals, this initiative laid the foundation for a more integrated approach to managing patients with serious cardiac illnesses. It underscored the importance of early palliative care involvement, empowering cardiology teams with the knowledge and skills to provide holistic, patient-centred care.
This inaugural teaching session was just the beginning. Since then, more than 15 MDT sessions have been conducted. The Cardio-Palliative Care initiative continues to evolve, with ongoing efforts to develop structured pathways, expand education, and implement nurse-led interventions to enhance cardio-palliative practice.
Each teaching session provided the team with valuable learning points that significantly enhanced patient care.
Feedback from participants Pre-and-Post MDT:
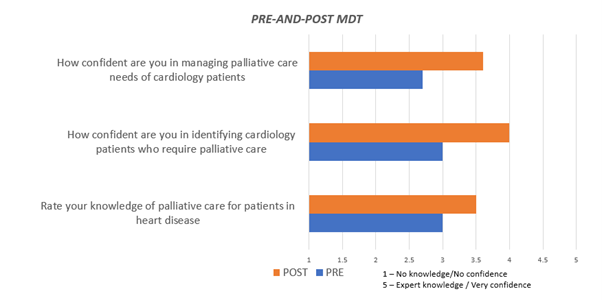
Confidence in Application Pre-and-Post MDT:
Palliative Care Resource Nurse (PCRN) Training
Introduction of PCRN Training Program
In April 2024, the Palliative Care Resource Nurse (PCRN) Training Program was launched in collaboration with the Intensive Care Unit (ICU) Nurses, with the aim to strengthen palliative care capacity within the Cardiology Department. This initiative helps equip nurses with essential knowledge and skills in symptom management and communication to ensure provision of holistic and compassionate care for patients with advanced cardiac conditions.
Why this Program is Essential
The PCRN program is a sustainable model for capacity building, empowering nurses to champion cardio-palliative care and improve outcomes for patients with advanced heart disease. This initiative marks a significant step in integrating palliative care into cardiology as a standard of care.
What is included in the Training Program?
The six-week structured curriculum covers key topics such as:
PCRNs: Bridging the Gap Between Cardiology and Palliative Care
PCRNs serve as key facilitators in integrating palliative care principles into cardiology practice. Some of their key contributions include:
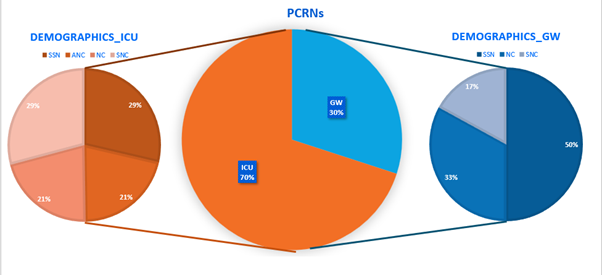
Who are the PCRNs?
Trained PCRNs: 6 nurses from the cardiac ICU were trained in the first cohort, bringing the total to 19 PCRNs being trained across NUHCS ICUs and general wards. There are also plans to expand the training to more batches in the future.
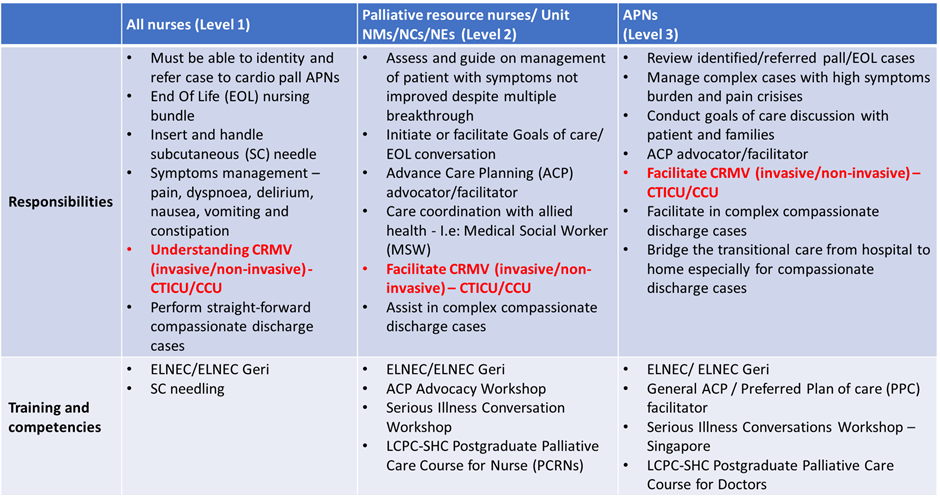
PCRN Responsibilities and Expected Training and Competency Level
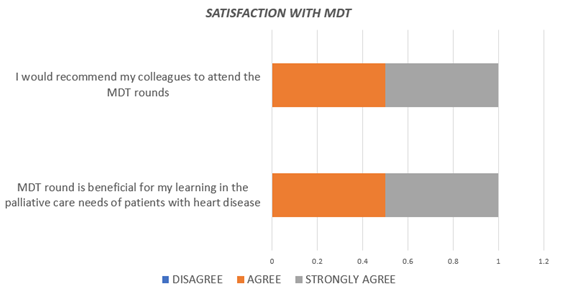
 Staff Feedback: Survey
Staff Feedback: Survey
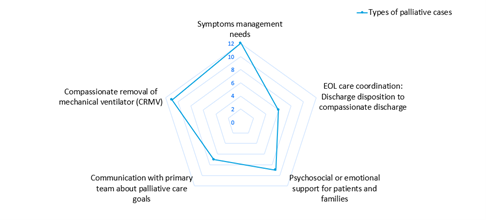
(i) Types of Palliative cases commonly managed by PCRNs
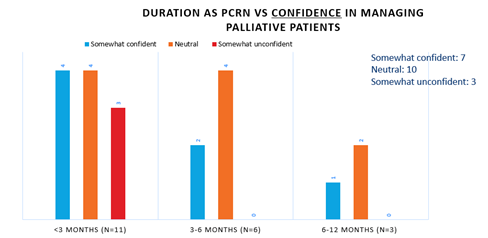
(ii) Confidence in Managing Palliative Patients
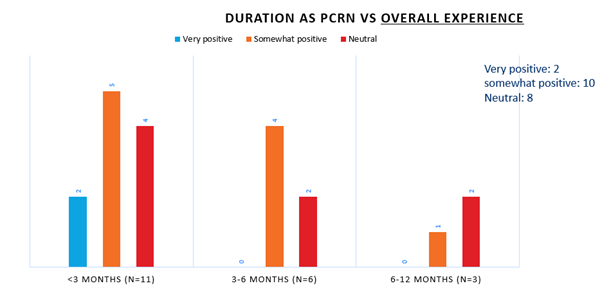
(iii) Overall Experience as PCRNs
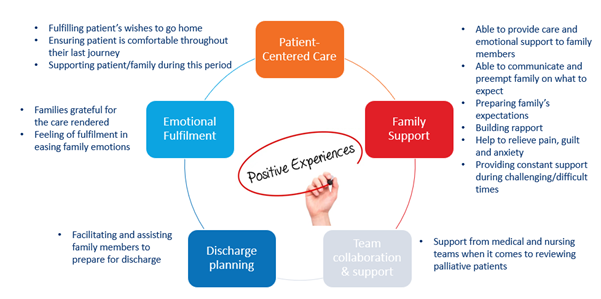
(iv) What are the Positive Experiences so far as a PCRN?
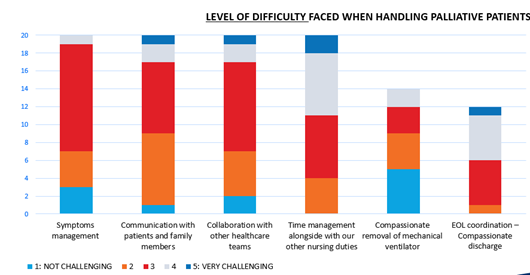
(v) Level of Difficulty Faced
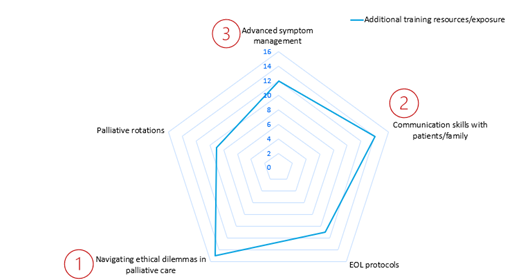
(vi) Additional training PCRNs
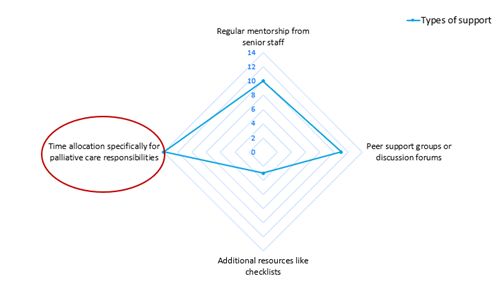
vii) Types of support PCRNs will need
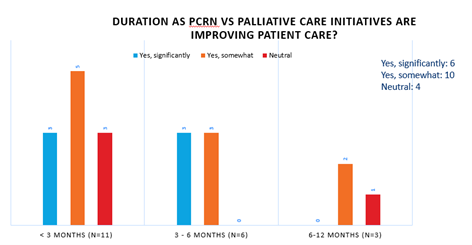
(viii) Overall feedback from PCRNs that this initiative/program is improving patient care
Compassionate Discharge
At NUHCS, the compassionate discharge process is a patient-centred initiative designed to allow terminally ill patients to spend their final moments at home. The PCRN plays a crucial role in this process, identifying potential candidates and initiating the process.
Cessation of inotropes and dialysis is a palliative initiative at NUHCS when active management is no longer beneficial to the patient. This process involves a coordinated multidisciplinary effort, with the critical care team working closely alongside cardiologists and nephrologists, to carefully taper inotropic support and discontinue dialysis. Clear communication with patients and families is paramount, ensuring their understanding and providing crucial emotional support throughout.
The PCRN conducts a thorough evaluation, communicating with patients, families, and respective member of the team to ensure the suitability of compassionate discharge. The team will then refer the patient to the palliative medicine team, leveraging their expertise in end-of-life care.
The PCRN then assists patients and their families in accordance with the Compassionate Discharge (ComD) bundle/protocol. This includes arranging home care services, providing education on symptom management, and ensuring all medical and logistical aspects are addressed.
This process exemplifies NUHCS' commitment to providing dignified, patient-centred care, allowing patients to spend their final days in familiar, comfortable surroundings with their loved ones.
Compassionate Cessation of Active Management
NUHCS implemented comprehensive palliative initiatives to ensure dignified end-of-life care when active management is no longer beneficial.
Compassionate Removal of Ventilation (CRMV) is the process of withdrawing mechanical ventilation support from a patient with the primary goal of providing comfort and dignity at the end of life, rather than prolonging life when further measures are deemed futile. A harmonised protocol across the different ICUs was developed and can be used in patients who are suitable for compassionate removal of both invasive and non-invasive ventilation. This process involves thorough discussion and preparation with the patient and family prior to withdrawing ventilatory support. Throughout the process, the primary team manages symptoms and alleviates distress based on the protocol.
Compassionate Removal of Extracorporeal Membrane Oxygenation (ECMO) is considered when the patient’s condition deteriorates despite ECMO support. The process begins with a thorough discussion with the patient (if possible) and family members to ensure their understanding and alignment with the decision. The process of withdrawing Extracorporeal Membrane Oxygenation (ECMO) support requires meticulous planning and execution by our multidisciplinary team, including intensivists, cardiac surgeons, medical social workers, nurses, and palliative care specialists. Throughout the process, we prioritize patient comfort, utilizing appropriate sedation and pain management strategies. Family members are kept informed and supported at every step.
Cessation of inotropes and dialysis is a palliative initiative at NUHCS when active management is no longer beneficial to the patient. This process involves a coordinated multidisciplinary effort, with the critical care team working closely alongside cardiologists and nephrologists, to carefully taper inotropic support and discontinue dialysis. Clear communication with patients and families is paramount, ensuring their understanding and providing crucial emotional support throughout.
As life-sustaining treatments are withdrawn, our focus shifts to prioritizing comfort and preserving the patient’s dignity. This initiative exemplifies our dedication to providing holistic, dignified care during the final stages of life, aligning medical interventions with the patient's goals and preferences.
Home Inotropes
Home parenteral inotropic infusion therapy serves as an option to improve heart failure symptoms in patients with end stage heart failure while allowing them to be at home and in the community. An infusion pump will be used to deliver medication to patients continuously via a Peripherally Inserted Central Catheter (PICC).
All patients who are deemed eligible by the Heart Failure on-call team:
Aim of therapy:
Collaboration with Home Hospice Team
NUHCS established valuable partnership with home hospice services, particularly Methodist Welfare Services (MWS), to enhance end-of-life care for heart failure patients. Dr Perryn Ng, clinician lead for cardio palliative initiatives, previously completed a clinical attachment with MWS, gaining crucial insights into their operations.
During this attachment, Dr Ng became aware that MWS covers the western area of Singapore, including the National University Health System (NUHS) catchment area. This geographical overlap creates an opportunity for seamless patient care transitions.
The collaboration enables NUHCS to refer heart failure patients requiring palliative care to MWS' home hospice services. This ensures patients receive specialized care in familiar surroundings. Additionally, NUHCS cardiologists and MWS hospice care professionals engage in regular discussion on the patients under their case, with the aim of improve the quality of life for patients with incurable heart conditions in their final stages of life.
Deactivation of Automated Implantable Cardioverter-Defibrillator (ACID) in End-of-Life Care
For patients nearing the end of life, deactivation of an AICD may be considered to prevent unnecessary shocks and discomfort. This process involves several key steps: