
Heart attack also known as myocardial infarct is usually caused by a blockage in blood supply to the heart muscles when the blood vessels supplying the heart (coronary arteries) are occluded. The most common causes are from atherosclerotic plaques (fatty deposits) built up within the lumen of the blood vessels, or from blood clots that block off the heart's blood supply (please see section on Coronary Artery Disease). Prompt treatment is of the essence to prevent progression to permanent damage to large areas of the heart.
Scar tissue will replace the heart muscle that dies as a result of the myocardial infarct.
Your doctor will diagnose a heart attack based on:
A combination of all of the above will lead to a definitive diagnosis of a heart attack.
The most common presenting symptom is central chest pain, which can occur both at rest and on exertion. The nature of this pain is more severe, and lasts longer than normal chest pain. The pain can travel up the jaw, to the left or both arms. It is often associated with sweating, shortness of breath, nausea, and/or vomiting. The patient may look pale as well. A smaller heart attack can be very similar to an episode of heartburn.
About one-fifth of patients, often the elderly and the diabetic, have no pain at all, and only present with symptoms of compromised heart function, such as shortness of breath, low blood pressure, palpitations/irregular heart rhythms (Please see section on Heart Arrhythmias).
A very severe heart attack can cause some patients to suddenly collapse and die.
An electrocardiogram (ECG or EKG) is a non-invasive test that measures the electrical activity of heartbeats. An electrical impulse travels through the heart with each beat. This impulse causes the heart muscle to squeeze and pump blood. An electrocardiographic machine detects these impulses and records them in the form of waves.
This test allows the doctors to evaluate the regularity of the patient's heart rhythm or abnormality, if any.
An ECG gives two major kinds of information. First, by measuring time intervals on the ECG, a doctor can determine how long the electrical wave takes to pass through the heart. Finding out how long a wave takes to travel from one part of the heart to the next shows if the electrical activity is normal or slow, fast or irregular. Second, by measuring the amount of electrical activity passing through the heart muscle, a cardiologist may be able to find out if parts of the heart are too large or are overworked.
No. There is no pain or risk associated with having an electrocardiogram. When the ECG stickers are removed, there may be some minor discomfort.
If you are outside of a hospital:
Once in a hospital:
The heart muscles that were affected during a myocardial infarct do not die off immediately. If the flow of blood and hence oxygen is restored to these muscles as soon as possible (within a few hours), much of the muscle cells will survive. This is the reason for prompt treatment. There are two ways in which this can be achieved:
As there may be increased risks of fatal heart arrhythmias developing after a heart attack, you may be transferred to the Coronary Care Unit (CCU) for closer monitoring and intervention if required. ECGs and blood tests will be carried out over the course of your stay to monitor your progress.
Once you are fit for discharge, you will need to control the risk factors of heart disease, such as stopping smoking, optimising diabetic control, and controlling the cholesterol levels in the blood. Drugs are also commonly prescribed to prevent a further myocardial infarct, and examples of them are aspirin (to make the blood "thinner" to prevent blood clots from forming), and a beta blocker (slows the heart rate down).
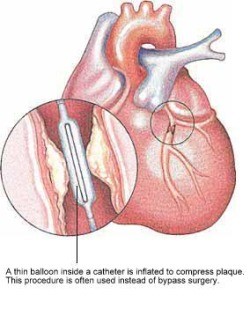
Coronary artery narrowings may be treated using either medications that reduce the heart's demand for blood, or by procedures aimed at increasing the heart's blood supply. One of the two most common methods to increase the blood supply is Coronary Angioplasty, sometimes abbreviated as PTCA (Percutaneous Translunimal Coronary Angioplasty).
PTCA offers a non-surgical alternative to Coronary Artery Bypass Surgery.
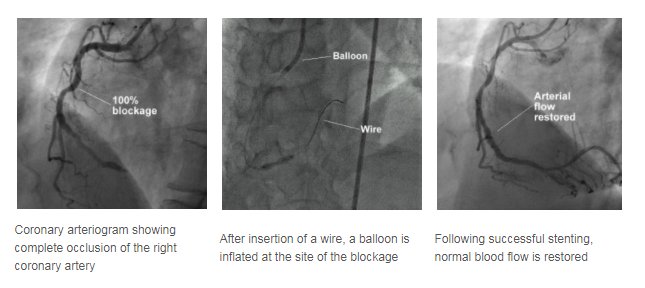
In PTCA, a balloon mounted on a thin tube (a catheter) is advanced into your coronary artery until it lies within the narrow area. The balloon is then inflated at high pressure, often a few times, to dilate the narrowing. Upon balloon deflation, the arterial narrowing is often significantly reduced.
A stent is a small metal coil to provide support to the narrowed segment of the coronary artery after angioplasty, preventing the artery from collapsing and reducing the likelihood that the narrowing will recur. Modern stents are made of stainless steel or a cobalt chromium alloy and are inert to the body. Some stents also have a medication coating and these may be preferred in certain situations to further reduce the chance of repeat narrowing of the heart arteries. Nowadays, stents are frequently placed directly over the narrowed segments (direct stenting) without prior balloon dilatation.

A stent is a small metal coil that provides support to the narrowed segment of the coronary artery after angioplasty.
Before going through a PTCA, a coronary angiogram is done first to provide a 'roadmap'. Undergoing PTCA is also very similar to having a coronary angiogram procedure.
During balloon inflation, you may experience some chest discomfort, and you should report this to your attending cardiologist. Stenting is carried out in a similar manner. The procedure may take 1 to 2 hours or more depending on the complexity of the diseased artery.
Following the successful PTCA, you will be monitored in a special monitoring ward. During this period, the sheath may be kept in your groin artery for 4 to 5 hours. However, the sheath may be removed immediately after the procedure if the situation allows. After the sheath is removed, the puncture site will be compressed for about 30 minutes to ensure that there is no bleeding.
You will have to remain in bed for several hours or until the following day to ensure the puncture site is sufficiently healed before walking. Your cardiologist will determine how long you need to stay in bed before you can walk around. Following that, some blood tests and ECGs will be performed to monitor your condition. If there are no complications, most patients can be discharged on the same day or the day after.
The success rate of coronary angioplasty is usually about 95%, depending on the nature of your coronary narrowing. However, in about 5% of cases, the procedure may be unsuccessful and the artery remains narrowed. In very few patients (about 1%), urgent bypass surgery may be required if the procedure is complicated.
There is a possibility of a recurrence of the narrowing of the coronary artery in the 6 months following the initial successful angioplasty or stenting, and you would usually feel a chest discomfort should it happen. If you feel a chest pain, you should seek medical attention immediately and inform your doctor.
Major complications like heart attacks, abnormal heart rhythm, stroke and death occurs in less than 1% of the patients undergoing PTCA.
Less serious complications like bleeding from the puncture site, bruising and swelling of the puncture site, and blood clot formation in the artery where the sheath is insert occurs in 1-3% of the patients.
Overall, the procedure is very safe and well-tolerated.
As a patient: