
Congenital means inborn or existing at birth.
Congenital heart disease or defect (CHD) is an abnormality of the structure of the heart that exists at birth. It occurs when the heart or major blood vessels fail to develop or mature normally during the pregnancy.
The list below describes some terms commonly used in CHD:
There are many different types of CHD that fall into four common categories of congenital defects:
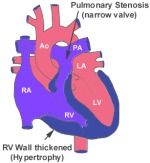
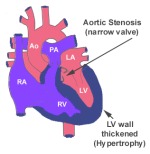
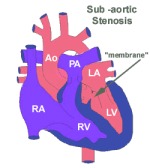
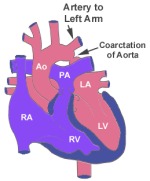
This occurs when either abnormally formed heart valves or major blood vessels block the flow of blood into or out off the heart such as:
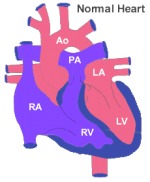
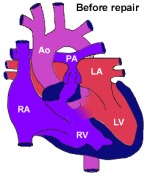
In a normal heart, the heart is made up of four chambers, two on either side, left and right. In simple terms, the left and right side of the heart are kept separated. The right side of the heart is responsible for receiving "used" blood (blood with reduced oxygen-blue blood) from the rest of the body and delivers it to the lungs. The left side of the heart is responsible for oxygen-rich blood - red blood from the lungs to send out to the rest of the body.
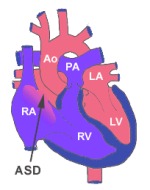
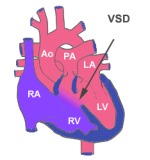
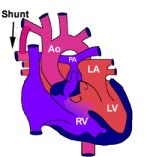
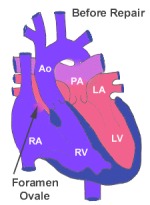
However, in left to right shunt types of CHD, the blood flows from left side of heart into right side of heart. This is due to abnormal connection between right and left side of the heart. This results in the right side becoming overloaded with "extra volume" of blood. When this happens, it results in too much blood flowing into the lungs.
In right to left shunts, the blood now flows from the right side of the heart to the left. This is also due to abnormal connection between the right and left side of the heart. It results in a decreased flow of blood into the lungs, which means that the amount of “used” oxygen depleted blood pumped into the lungs to be re-oxygenated reduces. This condition is also called “cyanotic heart disease” as this condition causes a bluish colour of the skin (usually in the tip of fingers and toes) and mucous membranes (lips) due to low oxygen levels in the blood.
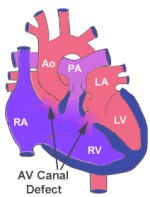
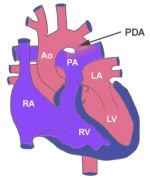
These defects have more than one defect and are also known as “mixing defects”.
Medical and surgical treatments now offer these children an opportunity to grow and mature into adult life, an option that was not available in the past once.
Accurate diagnosis is necessary for the doctor to give appropriate treatment.
Common tests used for diagnosis of CHD:
The presenting features of CHD depend on the age of your child and the type of defect present.
Common presenting features include:
If the condition is not corrected in a timely manner, damage to the heart and/or lungs could get beyond repair and consequently limit the life span of your child.
In some cases, CHD may be life-threatening and must be surgically corrected
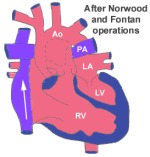
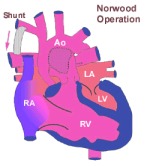
In other cases, the operation can be carried out after a few months or years, whilst in at times it is to repair the defect(s) in stages e.g.
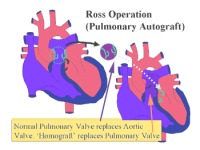
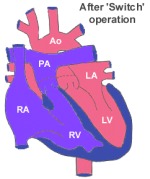
The following are some of the common paediatric heart surgical procedures.
Examples of conditions requiring open heart surgery:
Examples of condition for Closed Heart Surgery:
As a parent, you will be well informed of the risks and benefits of the surgery in advance so that you can make a decision with the help of the doctors.
Prior to your child’s discharge, he/she should be:
However, the surgical wound may get infected after discharge from the hospital.
You should contact the ward/doctors/nursing staffs to make an appointment for an earlier review if you:
The review can be arranged as soon as possible so that you can be reassured and any potential problems picked up well in advance.