
Atrial Fibrillation (AF) is the most common heart rhythm disorder – also known as arrhythmia - where there is very fast and disorganized contraction of the top chambers of the heart (atria) and causes an irregular heartbeat. This can affect the heart's pumping function leading to heart failure. Moreover, it can also cause blood to stagnate in the left atrium where it may form clots that could travel to the brain or elsewhere causing strokes or damage to other organs. AF is a progressive condition, meaning that if it is not treated, it can worsen. When this occurs, episodes tend to become more frequent and last longer
AF results in:
Types of AF:
Paroxysmal AF
Persistent AF
Many people do not know how they have AF, but it is most often caused by a combination of factors. Even people committed to healthy lifestyles and who have no other medical problems can develop AF.
Possible heart health factors:
Behaviours that may be associated to a risk in developing AF:

AF is diagnosed on an electrocardiogram (ECG), which is a test performed in the clinic that records electrical activity of the heart to detect cardiac problems. AF can also be diagnosed by mobile devices that are worn by the patient to monitor the heart over longer periods of time. These include Holter monitors and smart watches with ECG functionality.
If possible, we aim to restore the heart's normal rate and rhythm, and this is done with medications and/or procedures. Most AF patients also need medications to lower stroke risks.
Medications are prescribed for a reason. Always take them as prescribed and speak to your doctor before making any consumption changes. It is crucial for you and your doctor to communicate accurately about your health risk level. Without risk-lowering treatment, nearly 35% of AF patients eventually suffer from a stroke.
Stroke risk reduction is achieved predominantly through the use of medication called anti-coagulants which reduce the clotting ability of the blood and therefore the likelihood of clot formation and by extension the risk of these clots migrating to the brain and causing a stroke. The risk of bleeding is inescapably elevated with the use of these drugs. Hence the risk of stroke vis-à-vis the risk of bleeding has to be considered before deciding to commence on anticoagulation. In patients in whom there is contraindication to anticoagulation in the setting of high stroke risk, left atrial appendage occlusion can be considered.
How to spot stroke FAST?
Heart failure prevention is achieved mainly through the use of medications to control the heart rate (ventricular rate) so that it is not persistently elevated heart rates. Other medications may be prescribed to reduce the probability of heart muscle damage.
Restoration and maintenance of normal heart rhythm can be achieved through the use of specific drugs called "anti-arrhythmic drugs" (AADs) or through an ablation procedure.
Generally, AADs may reduce the episodes and duration of AF but do not eliminate or "cure" AF. There can also be side-effects resulting from the use of these drugs.
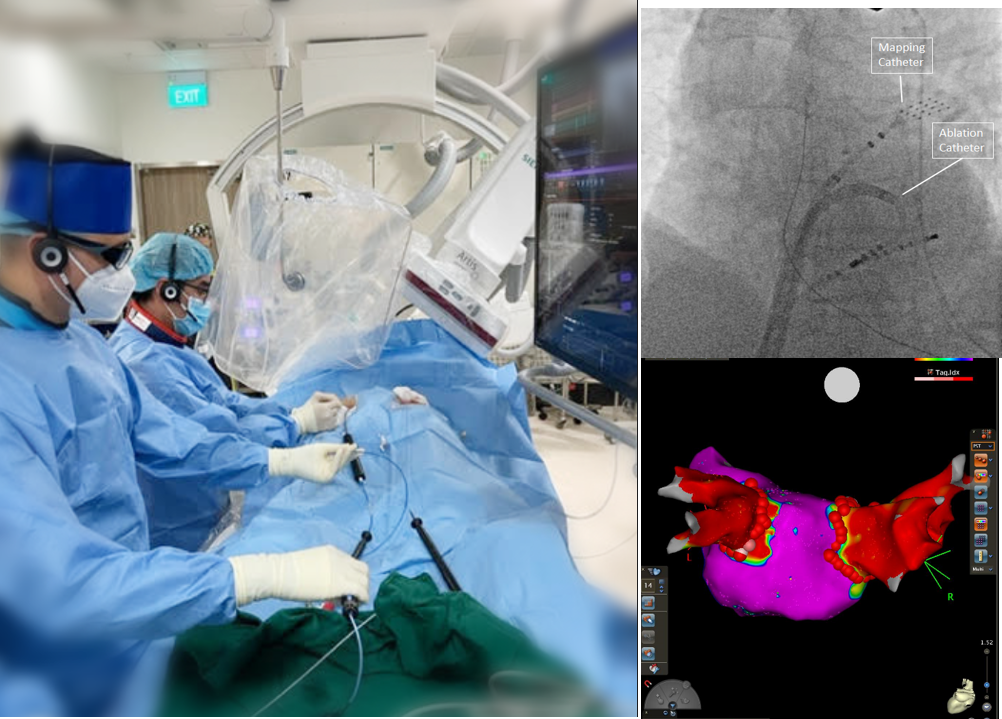
Catheters are positioned in the heart via the blood vessels in the groin under x-ray guidance, allowing your doctor to create a 3-dimensional virtual map of your heart to localise the heart rhythm abnormality.
As an AF patient, even if I do not exhibit any noticeable symptoms, am I still at risk for stroke?
Yes! Do not stop taking medication simply because you are not experiencing noticeable symptoms. Many people with AF should be on anticoagulant medications which will lower stroke risks when taken correctly.
Let your doctor know if you are having symptoms and continue following your doctor's orders until otherwise directed.
Watch the video below to know more about stroke prevention:
Does having AF mean I need to wear a medical alert bracelet or carry a card in my wallet?
In any emergency situation, having a patient's medical history is very helpful. Be sure and write down the medication that you are taking and the dosage. If you are taking oral anticoagulant medications ("blood thinners"), always wear a medical alert bracelet or carry a wallet card for healthcare providers to be aware of your condition and provide the best care for you, should an emergency occur.
Can I tell when I'm going to have an episode of AF?
Some people can tell when they are having an episode of AF while others do not. Either way, you may be able to control the "triggers" that can cause your AF to flare up, and these "triggers" may be different for different people. Common triggers may include caffeine, excessive alcohol, stress, poor sleep, and, for some people specifically, exercise that increases the heart rate above a certain point. Despite that, it is important to note that exercise is actually beneficial for many people with AF.
Am I able to have sex or exercise?
Yes, as long as you are cleared by your doctor, you are able to perform any normal activities of daily living that you are able to tolerate.
Can I drive my car?
Most people with AF are able to, but do check in with your doctor. Some people experience dizziness or even fainting with their AF episodes. If you feel dizzy or lightheaded, pull over to the side of the road and stop. Discuss with your healthcare provider to understand when your AF symptoms need to be assessed by a medical professional.
Is AF curable or is it a permanent condition?
Although AF is not traditionally known to be entirely curable, in some cases, the condition can be treated to significantly lessen the amount of AF that you have. Medications and procedures that control the heart rate and rhythm can also help lower stroke risks. AF, regardless of the duration, needs to be monitored by a doctor. There are different classifications of AF – from paroxysmal, persistent, longstanding persistent to permanent. The treatment plans and outcomes may depend on several factors, including the type of AF. Regular check-ups to monitor the condition and keep risks low is crucial.
Can I die from an episode of AF?
Generally, no. AF, by itself, is usually not deadly but a stroke caused by AF can be life-threatening. People who have AF are at an increased risk for stroke and other heart-related complications like heart failure. The most important thing you can do is to work with your doctor or other healthcare providers to ensure that you are doing all you can to prevent any complications that could occur as a result of having AF.
Can I live a long life with AF?
People can live long, healthy and active lives with AF. Controlling your risk factors for heart disease and stroke and knowing what can possibly trigger your AF will help improve your long-term management of AF. It is important to work with your doctor who can help you in managing this condition through the different stages of your life.
Keen to find out more on Living with AF? Check out the video below: