Overview
Acute myocardial infarction (AMI) or 'heart attack' is one of the top ten leading causes of death in Singapore. It occurs when there is sudden blockage caused by a thrombus (clot) in a diseased coronary artery, resulting in oxygen depletion to the affected area. If not treated promptly, permanent heart damage or even death ensues.
The modes of treatment for acute myocardial infarction have changed over the decades - from drugs that function to lyse or dissolve the clot, or dilate the lumen of small blood vessels, to procedures that pass a catheter through a vessel in the groin or wrist all the way into the heart vessels to relieve the obstruction with the use of 'balloons' and/or 'stents'.
This review covers the components of optimal AMI care that NUH has been monitoring and reviewing with the ultimate goal of providing the best AMI care for their patients.
'When time is of essence'
In AMI, every minute counts - from the onset of symptoms, to recognition of the disease to the appropriate measures instituted by the physician. Most commonly, it presents as chest pain, or less typically, jaw pain, upper mid-abdominal (epigastric) discomfort, and shortness of breath.
International bodies like the Institute of Healthcare Improvement (IHI) and the Joint Commission International (JCI) have identified Quality Measures that can focus on these timely interventions that can help regain normal blood flow into the heart tissues.
The Key Components of AMI Care:
Aspirin on arrival
The use of aspirin within 24 hours before or after hospital arrival, results in a significant reduction in vascular events and subsequent mortality. Clinical guidelines strongly recommended early aspirin for AMI patients without contraindications. Aspirin acts within minutes to prevent additional platelet activation and interferes with platelet adhesion and cohesion.
Over the past 10 years since 2011, all patients have been given aspirin on arrival.
Aspirin prescribed at discharge
Aspirin therapy in patients, who have suffered from AMI, reduces the risk of vascular events and mortality by 20%, according to the Antiplatelet Trialists' Collaboration. Long-term aspirin therapy for the secondary prevention of subsequent cardiovascular events in patients discharged after an AMI.
We have steadily increased our rates since the initiative started and have achieved 100% compliance since 2011.
Beta blocker at discharge
The use of beta-blockers for AMI patients can reduce mortality and morbidity. Long-term use after an AMI episode has also been shown to reduce mortality by 23%. It is thus recommended for the secondary prevention of subsequent cardiovascular events in patients discharged after an AMI.
ACE Inhibitors or ARB for LVSD
The use of angiotensin converting enzyme inhibitor (ACE-I) in patients with both S-T elevated myocardial infarction (STEMI) and non-ST elevated myocardial infarction (NSTEMI) who have left ventricular systolic dysfunction (LVSD), has been shown to decrease mortality rates. Angiotensin receptor blockers (ARB) may be used for patients who are intolerant to ACE inhibitors. It is recommended for AMI patients with LVSD with ejection fraction of less than 40%.
Since 2017, 100% of patients were prescribed ACE inhibitors or ARB upon discharge.
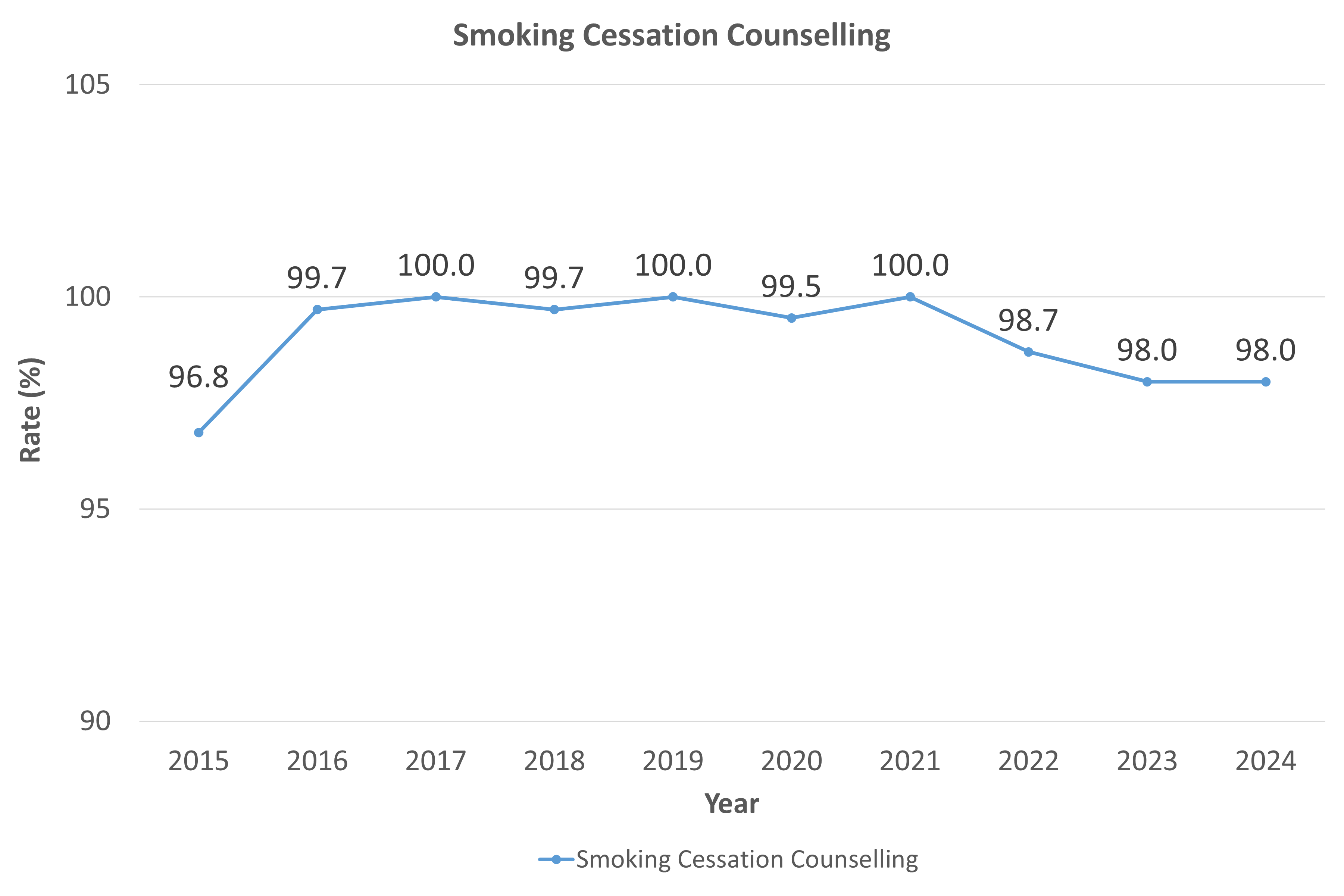
Smoking cessation counselling
Smoking is a major risk factor for coronary heart disease and eventually AMI. Smoking cessation thus reduces morbidity and mortality in all populations. It is recommended to give smoking cessation advice to smokers hospitalised with AMI. They should also be offered smoking cessation resources, like nicotine replacement therapy.
Measures towards increasing smoking cessation counselling are being undertaken.
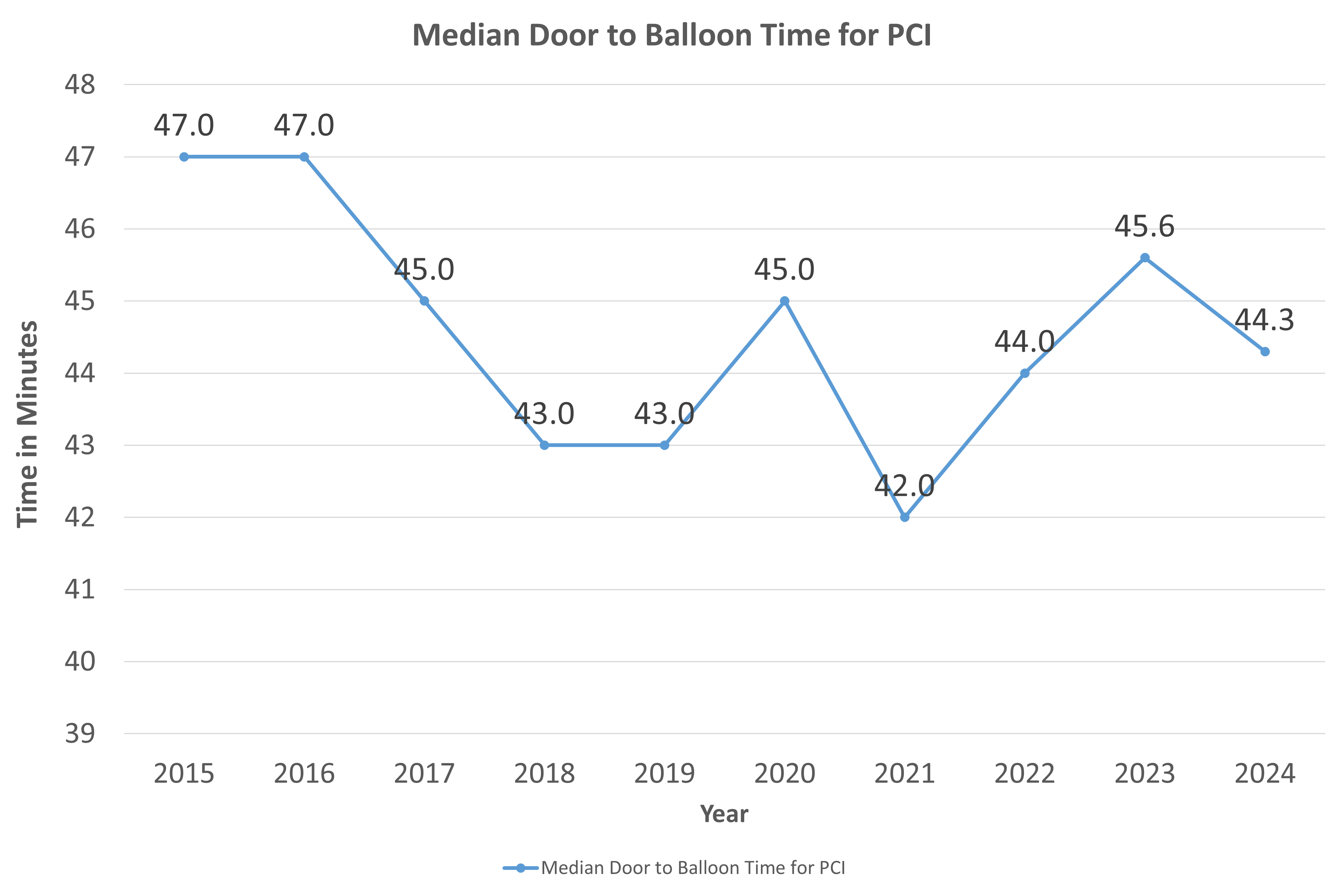
Door-to-balloon time
Percutaneous coronary intervention (PCI) is a treatment modality that mechanically clears occluded culprit coronary artery. Dubbed as "door-to-balloon time", this quality measure is a key process indicator in that time is really of major essence. A target time of 120 minutes, but a "stretch target" of 90 minutes is recommended. The earlier the intervention is done, the faster is the recovery of injured heart muscles. However, one must take note that only those patients whose electrocardiogram (ECG) shows an ST-elevated myocardial infarction (STEMI) benefit from this procedure.
We adopt a stretch target of 90 minutes. For this indicator, our rates are steadily improving over time.

Conclusion
We are continuously reviewing these measures in the pursuit of giving the best quality care to its AMI patients. By implementing process improvements at every step in a patient's journey through the hospital, quality of care is evident in our key AMI care components.
References: